Neuroophthalmology
Dr.
Sharpe
May 13, 2005
Visual field defects
Visual field testing
- visual acuity-corrected – with glasses
- finger counting – counting fingers in each quadrant
- hand comparison and colour comparison
- Amsler grid – for central 10 degrees
grid of 20 degrees, broken or wave lines or a hole if pathological - perimetry
- Humphrey – usually central 30 degrees – static perimetry
- Goldmann perimetry – entire field – kinetic perimetry
- Tangent screen (seldom used)
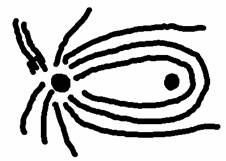
Visual field defects in retinal disease
- constriction – pigmentary retinopathies, e.g., retinitis pigmentosa
- scotomas
o punctuate – blob – e.g. retinal hemorrhage
o ring- pigmentary retinopathies
o arcuate – nerve fiber layer infarct
- depression
Nerve fiber layer:
54% fibers cross at optic chiasm, 46% don’t cross.
Chiasmal field defects
- anterior angle syndrome
o junctional scotoma
o monocular temporal hemianopia
- median bar syndrome
o bitemporal upper field defect
- upper chiasm 3rd ventricle masses
o lower bitemporal field loss
Optic tract and geniculate defects
- incongruous homonymous hemianopia with RADP in opposite eye – optic tract lesion
- geniculate characteristic effects
o sectoranopias – congruous
§ sparing vertical meridian – lateral choroidal artery occlusion
§ sharing horizontal meridian – anterior choroidal artery occlusion
Temporal lobe “pie in the sky” defect (upper temporal field defect) due to Meyer’s loop in the temporal lobe.
Lesions of the optic radiation are usually congruous. If upper tracts affected, lower field defect, and vice versa.
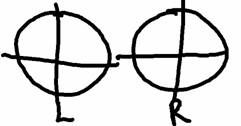
This is the convention for drawing visual fields:
Holmes map of primary visual cortex – V1
- 25% of the striate cortex was assigned to the central 15 degrees of vision.
- Actually first described by a Japanese scientist, “Innue?”
- Depth of calcarine fissure is the horizontal meridian of the visual field
- Upper lip of calcarine cortex represents the lower limit of the visual field
- Anterior portion of the calcarine cortex includes the vertical meridian
Constricted visual fields
- bilateral occipital infarction
- tapetoretinal degenerations (retinitis pigmentosa)
- glaucoma
- atrophic papilledema
- optic nerve drusens (hyaline bodies)
- functional (conversion disorder or malingering)
o functional defect stays same size regardless of distance
Optic neuropathies
Optic neuropathies
- acute optic neuritis
- (papilledema)
- anterior ischemic optic neuropathy
- compressive optic neuropathies
- infiltrative optic neuropathies
- toxic and nutritional
- hereditary
Acute optic neuritis
- inflammatory, mostly commonly demyelination
- can be associated with other diseases
- acute or subacute visual loss
- visual field defects, RAPD
- ocular/periorbital pain on eye movement
- disk hemorrhages are uncommon
- maximal visual loss in 1-2 weeks
- improvement within 4 weeks
Anterior optic neuritis = papillitis
Retrobulbar optic neuritis = normal disk or later pallor/atrophy
Neuroretinitis – associated with macular star (not MS, usually idiopathic/viral/cat scratch)
According to the Optic Neuritis Treatment Trial, without MRI lesions, likelihood of developing clinically definite MS in 10 years is 23% after optic neuritis. IFN beta 1a decreases likelihood of progression to MS. Steroids speeds recovery somewhat, but does not affect final result. Can use steroids to delay diagnosis at 2 years. IV methylprednisolone 1g/d x3days, avoid just oral prednisone, but do taper.
DDx of optic neuritis:
- idiopathic/demyelination
- SLE
- other vasculitides
- sarcoidosis
- syphilis
- Lyme disease
- viral/post-viral
- other infectious/inflammatory disorders
Incidence so low, no need to do blood tests initially. Consider if not getting better in a few weeks.
Papilledema
- optic disc edema due to increased ICP
- typically bilateral, but often assymetrical
- blockage of axoplasmic flow
- bilateral disc elevation, obscuration of disc margins/blood vessels, venous distension/tortuosity, absent spontaneous venous pulsations
- (nasal and upper poles can often not be clear margins)
- Venous pulsations means the ICP is <200
Stages of papilledema
- early – hyperemia, superior/inferioredema
- acute – hemorrhages, infarcts, retinal folds (Paton’s rings)
- chronic – “champagne cork” appearance, optociliary shunts
- atrophic – pallor, arteriolar narrowing
Clinical features of papilledema
- signs and symptoms of increased ICP
- transient visual obscurations (TVOs)
- relative sparing of central acuity
- enlarged blind spots, constriction of VF
Papilledema DDx:
- intracranial mass
- CVST
- Intracranial hemorrhage
- Hydrocephalus
- Meningitis
- Spinal cord tumour
- GBS, CIDP
- Dural AVM
- Idiopathic intracranial hypertension (pseudotumour cerebri)
Pseudopapilledema
- congenital anomaliesm mimic papilledema
- asymptomatic, often without headache
- anomalous vascular branching
- tilted discs, optic disc drusen
- bilateral in 2/3 cases
Maligctioarnant hypertension
- disc swelling mimics papilledema
- Elevated BP
- Encephalopathy not always present
- Cotton wool spots, macular lipid star
- Typically hemorrhagic retinal away from disc
Anterior ischemic optic neuropathy
- most common in patients >50 years
- sudden, unilateral visual loss
- presumed optic head ischemia
- sparing of central retinal artery, infarction of small ciliary arteries
- pale swelling
Giant cell arteritis (arteritic ION)
- true emergency
- HA, jaw claudication, scalp tenderness (not required)
- Elevated ESR, CRP
- Bilateral or sequential, amaurosis fugax
- 90% anterior or posterior ION, 3-5% central retinal artery occlusion, ocular ischemia, double vision (brainstem, eye muscles)
- Treat first, biopsy temporal artery later – IV methylprednisolone 1g/day x3days then oral 1-2 years, goal to protect fellow eye
- Can biopsy up to 2 weeks into steroid treatment
Central retinal artery occlusion
- branch vs. central
- retinal whitening “cherry red spot”
- if there is a cilioretinal artery, you can spare the macula (no cherry red spot)
- prognosis is poor even with treatment
- paracentesis, ocular massage, lower IOP, heparin (IA thrombolysis), work up for underlying etiology
Compressive optic neuropathies – the big 4
- pituitary adenoma
- meningioma – sphenoid or clinoid
- giant aneurysm – carotid ophthalmic
- craniopharyngioma